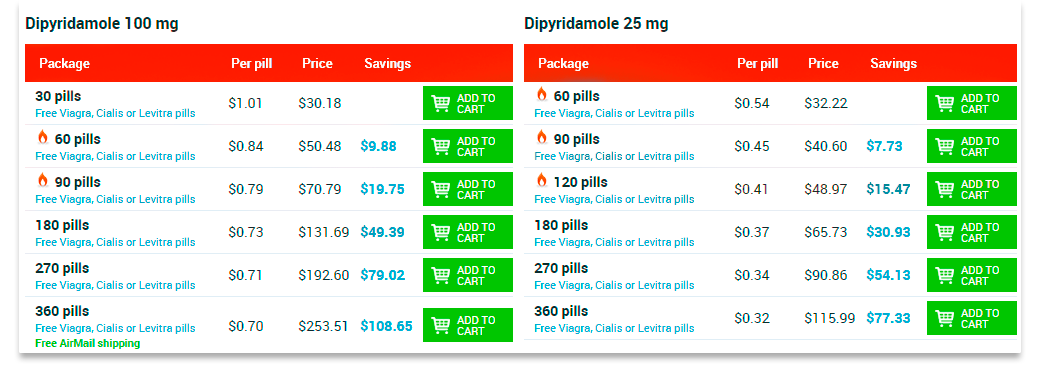
BUY DIPYRIDAMOLE ONLINE USA
Dipyridamole is an immunomodulating drug that improves microcirculation
Pharmacological properties.
Pharmacodynamics.
Expands coronary vessels (mainly arterioles) and causes a significant increase in the volume flow rate. Increases the oxygen content in the venous blood of the coronary sinus and its absorption by the myocardium. Promotes the development of collateral coronary circulation, reduces the overall peripheral vascular resistance, improves microcirculation, has an angioprotective effect. These effects are due to the increased activity of endogenous adenosine due to a decrease in its capture by tissues and destruction (adenosine affects the smooth muscle of blood vessels and prevents the release of norepinephrine).
It is an antagonist of the endogenous ADP aggregate, inhibits PDE, thus reducing the release of platelet aggregation activators - thromboxane, ADP, serotonin, etc., increases the synthesis of prostacyclin I2 with endothelium of the vascular tissue, which inhibits platelet aggregation. Reduces adhezivnost platelets, prevents the formation of clots in the blood vessels and reduce blood supply in the source of ischemia. Antiaggregant effect occurs at a plasma concentration of 0.1 μg / ml. As an antiplatelet drug is often used in combination with acetylsalicylic acid. Dose-dependent extends the abnormally shortened lifetime of thrombocytes.
Expands coronary arteries, especially unchanged, causes the phenomenon of stealing. It is an interferon inducer, has a modulating effect on the functional activity of the interferon system, increases the decreased production of interferon alpha and gamma-leukocytes in vitro. Increases nonspecific antiviral resistance to viral infections.
Normalizes venous outflow, reduces the incidence of deep vein thrombosis in the postoperative period. Improves microcirculation in the retina of the eye, renal glomeruli. Reduces the tone of the cerebral vessels, it is effective for dynamic disorders of cerebral circulation. According to the angiographic study, the combination of acetylsalicylic acid with dipyridamole slows the progression of atherosclerosis.
In obstetric practice, corrects placental blood flow, prevents dystrophic changes in the placenta (with the threat of preeclampsia), eliminates hypoxia of the fetal tissues and promotes the accumulation of glycogen in them.
Pharmakokinetics.
When taken orally, it is rapidly absorbed within 45-75 minutes, mainly in the stomach, a small part - in the small intestine. Bioavailability is 37-66%. The maximum concentration is recorded after 1 hour after administration. The degree of binding to plasma proteins is 91-99% (mainly with albumin and acid alpha-glycoprotein). Quickly penetrates into the tissue. Accumulates, first of all, in the heart and red blood cells. Metabolized mainly in the liver. It is excreted with bile in the form of glucuronides. Renal elimination is not significant. When the liver is impaired, cumulation is possible. The half-life of the drug varies depending on the individual characteristics of the patient and is 6-8 hours.
Clinical characteristics.
References.
Prevention of arterial and venous thrombi, including after surgery for prosthetic heart valves. Prevention of occlusion of stents and aortocoronary shunts (in combination with acetylsalicylic acid).
Treatment and prevention of cerebral circulation disorders according to the ischemic type.
Disturbances of microcirculation of any genesis (as part of complex therapy), chronic obliterating diseases of the vessels of the lower extremities, especially in the presence of risk factors (arterial hypertension, smoking).
3 Contraindications. Hypersensitivity to the components of the drug. Acute myocardial infarction. A common severe atherosclerosis of the coronary arteries. Unstable angina. Hypertrophic obstructive cardiomyopathy. Decompensated chronic heart failure. Arterial hypotension. Hemorrhagic diathesis. Stomach ulcer and duodenal ulcer (with a predisposition to bleeding). Chronic obstructive pulmonary disease. Chronic renal failure. Liver failure. Children under 12 years.
2 Mode of administration and dose. Apply inside. Assign adults and children over 12 years of 1-2 tablets (25-50 mg) 3 times a day. If necessary, the dose can be increased to 3 tablets (75 mg) at the reception 3 times a day. The maximum daily dose is 600 mg. The drug is used for 1 hour before eating, without chewing and squeezed a small amount of liquid.
The duration of the course of therapy is set individually and, as a rule, ranges from several weeks to several months.
Feather reactions.
From the cardiovascular system: a feeling of palpitations, tachycardia, bradycardia, blood flow to the face, coronary steal syndrome (when doses more than 225 mg / day). Reduced blood pressure.
From the digestive system: nausea, vomiting, diarrhea, epigastric pain. The possible reaction frequency is about 6%.
On the part of the blood and hemostasis system: thrombocytopenia, changes in the functional properties of platelets, bleeding, increased bleeding.
Other: weakness, dizziness (up to 13%), sensation of stuffiness in the ears, head noise, headache, hyperemia of the skin of the face, arthritis, myalgia, rhinitis, alopecia.
Allergic reactions: skin rashes (2.3%).
Overdose.
Symptoms.
Feeling of hot flushes to the face, increased sweating, weakness, dizziness, anxiety, lowering of blood pressure, tachycardia. In severe cases, hemorrhage.
Treatment.
Gastric lavage to remove the remnants of the dosage form. A suspension of activated carbon inside. Further treatment is symptomatic. Hemodialysis is ineffective due to the strong binding of dipyridamole to plasma proteins.
2 Application during pregnancy or lactation. Adequate and strictly controlled studies on efficacy and safety in pregnant women have not been conducted. Use during pregnancy is possible if the expected benefit to the mother exceeds the potential risk to the fetus.
The drug penetrates into breast milk, in connection with which it is necessary to solve the problem of stopping breastfeeding.
Features of application.
To reduce the dyspeptic phenomena are taken with milk. In the treatment should be avoided the use of natural coffee and tea, weakening the effect of dipyridamole.
The ability to influence the speed of reactions when driving vehicles or other mechanisms. The drug should be administered with caution to persons who manage motor vehicles and work with potentially dangerous mechanisms.
2Interaction with other drugs and other interactions. The antiaggregant effect of dipyridamole is increased with the use of indirect anticoagulants, acetylsalicylic acid, penicillin series antibiotics, cephalosporins, tetracyclines, chloramphenicol, nicotinic acid.
The xanthine derivatives containing caffeine weaken the antithrombotic effect of dipyridamole.
Dipyridamole weakens the effect of cholinesterase inhibitors.
Beta-lactam antibiotics, tetracyclines and chloramphenicol increase the effect of dipyridamole.
Antacids reduce its maximum concentration due to reduced absorption.
Heparin, indirect anticoagulants, thrombolytics increase the risk of hemorrhagic complications.
Why is the lack of blood supply to the brain?
Acute violation of cerebral circulation according to the ischemic type is more often a secondary pathology, arises against the background of existing diseases:
- arterial hypertension;
- widespread atherosclerotic vascular disease (up to 55% of cases develop due to severe atherosclerotic changes or thromboembolism from plaques located in the aortic arch, brachiocephalic trunk or intracranial arteries);
- suffered myocardial infarction;
- endocarditis;
- heart rate abnormalities;
- changes in valvular heart apparatus;
- vasculitis and angiopathy;
- vascular aneurysms and developmental anomalies;
- blood diseases;
- diabetes mellitus.
Up to 90% of patients have changes in the heart and the main arteries of the neck. The combination of these causes dramatically increases the risk of ischemia.
Syndrome of the vertebral artery
Perhaps the compression of the vertebral artery by the processes of the vertebrae
The reason for transient attacks is often:spasm of the arterial trunk of the brain or short-term compression of the carotid, vertebral arteries;
embolization of small branches.
The following risk factors may provoke the disease:
- elderly and senile age;
- excess weight;
- the effect of nicotine on blood vessels (smoking);
- stresses.
The basis of the acting factors is the narrowing of the lumen of blood vessels, through which blood flows to the cells of the brain.
However, the consequences of such a disturbance of nutrition can be different in:
- firmness,
- localization,
- prevalence,
- the severity of the stenosis of the vessel,
- severity.
The combination of factors determines the form of the disease and the clinical symptoms.
 Ischemic stroke can be considered recurrent if it occurs in the blood supply zone of one vessel within 28 days after the initial manifestations of the first case. A repeat is called a stroke at a later date.
Ischemic stroke can be considered recurrent if it occurs in the blood supply zone of one vessel within 28 days after the initial manifestations of the first case. A repeat is called a stroke at a later date.
Pathogenesis of different forms of acute cerebral ischemia
Transient ischemic attack was formerly called transient impairment of cerebral circulation. It is isolated in a separate form, since it is characterized by reversible disorders, the focus of the infarction does not have time to form. Usually the diagnosis is put in retrospectively (after the disappearance of the main symptomatology), in a day. Until then, the patient is being treated like a stroke.
The main role in the development of hypertensive cerebral crises belongs to an increased level of venous and intracranial pressure with damage to the walls of the vessels, the release of fluid and protein into the intercellular space.
insult of the brain
The edema of the brain tissue in this case is called vasogenic
The feeding artery is necessarily involved in the development of ischemic stroke. The cessation of blood flow leads to oxygen deficiency in the outbreak formed in accordance with the boundaries of the basin of the affected vessel.
Local ischemia causes necrosis of the area of the brain tissue.
Depending on the pathogenesis of ischemic changes, types of ischemic strokes are distinguished:
atherothrombotic - develops in violation of the integrity of the atherosclerotic plaque, which causes complete closure of the internal or external feeding cerebral arteries or their sharp narrowing;
cardioembolic - the source of thrombosis is the pathological growths on the endocardium or heart valves, fragments of the thrombus, they are delivered to the brain with a general blood flow (especially when the oval hole is not open) after attacks of atrial fibrillation, tachyarrhythmia, atrial fibrillation in patients in the post-infarction period;
lacunar - more often occurs when small intracerebral vessels are affected in arterial hypertension, diabetes mellitus, small focal size (up to 15 mm) and relatively small neurological disorders;
hemodynamic - cerebral ischemia with a general decrease in the rate of circulation and a drop in pressure on the background of chronic heart diseases, cardiogenic shock.2 Cardiovascular diseases
In cases of hemodynamic disorders, the blood flow in the brain vessels may decrease to a critical level and lower
It is worth explaining the variant of the development of strokes of unknown etiology. This happens more often if there are two or more reasons. For example, in a patient with carotid artery stenosis and fibrillation after an acute infarction. It should be borne in mind that elderly patients already have stenosis of the carotid arteries on the side of the alleged disorder caused by atherosclerosis, in the amount of up to half the lumen of the vessel.
Star infarction of the brain
Stages of pathological changes are allocated conditionally, they are not necessarily present in each case:
Stage I - hypoxia (oxygen deficiency) disrupts the permeability of the endothelium of small vessels in the outbreak (capillaries and venules). This leads to the transition of fluid and protein of blood plasma into the brain tissue, the development of edema.
II stage - at the level of the capillaries, the pressure continues to decrease, which disrupts the functions of the cell membrane, nerve receptors on it, electrolyte channels. It is important that all the changes so far are reversible.
III stage - the metabolism of cells is disrupted, lactic acid accumulates, a transition to the synthesis of energy occurs without the participation of oxygen molecules (anaerobic). This species does not allow maintaining the necessary level of life of cells of neurons and astrocytes. Therefore, they swell, cause structural damage. Clinically expressed in the manifestation of focal neurological signs.
What is the reversibility of pathology?
For timely diagnosis it is important to establish a period of reversibility of symptoms. Morphologically this means the stored functions of the neurons. The brain cells are in the phase of functional paralysis (parabiosis), but they retain their integrity and usefulness.
Ischemic stroke
The ischemia zone is much larger than the site of necrosis, the neurons in it are still alive
In an irreversible stage, you can identify a zone of necrosis in which the cells are dead and can not be repaired. Around it is a zone of ischemia. The treatment is aimed at supporting the full nutrition of neurons in this zone and at least a partial restoration of the function.
Modern research has shown extensive connections between brain cells. A person does not use all his reserves and opportunities for his life. Some cells are able to replace the deceased and provide their functions. This process is slow, so doctors believe that the rehabilitation of a patient after an ischemic stroke should continue for at least three years.
Signs of impending circulatory disorders of the brain
B, the clinicians attribute to the group of transient disorders of cerebral circulation:
- transient ischemic attacks (TIA);
- hypertensive cerebral crises.
Features of transient attacks:
- by duration fit within a period of several minutes to a day;
- one in ten patients after TIA during the month there is ONMK on ischemic type;
- Neurologic manifestations are not gross in nature;
- light manifestations of bulbar paralysis (foci in the brainstem) with oculomotor disorders are possible;
- visual impairment in one eye in combination with paresis (loss of sensitivity and weakness) in the extremities of the opposite side (often accompanies incomplete narrowing of the internal carotid artery).3 It is important!
Head of the Institute of Cardiology recommends the treatment of bad cholesterol to get rid of cardiovascular diseases ...
Features of hypertensive cerebral crises:
the main manifestations are cerebral symptoms;
Focal features are rare and mild.
Patient complains about:
a sharp headache, more often in the nape, temples or crown;
state of deafness, noise in the head, dizziness;
nausea, vomiting.
Encoupling:
temporary confusion of consciousness;
excited state;
sometimes - a short-term attack with loss of consciousness, seizures.
Transient disturbances are not accompanied by any deviations in computer and magnetic resonance imaging, since there are no organic changes.
Signs of a cerebral stroke
Ischemic stroke means the occurrence of irreversible changes in the brain cells. In the clinic, neurologists distinguish the periods of the disease:
- acute - continues from the onset of manifestations within 2-5 days;
- acute - lasts up to 21 days;
- early recovery - up to six months after the elimination of acute symptoms;
- late recovery - takes from six months to two years;
- consequences and residual events - over two years.
Some doctors continue to allocate small forms of stroke or focal. They develop suddenly, the symptomatology does not differ from cerebral crises, but lasts up to three weeks, then completely disappears. The diagnosis is also retrospective. During the examination, no organic abnormalities are detected.
Brain ischemia, in addition to general symptoms (headaches, nausea, vomiting, dizziness), is localized. Their character depends on the artery, which is "off" from the blood supply, the state of collaterals, the dominant hemisphere of the brain in the patient.
Consider the zonal signs of occlusion of the cerebral and extracranial arteries.
When the internal carotid artery is injured:
- impaired vision on the side of blockage of the vessel;
- the sensitivity of the skin on the limbs, the face of the opposite side of the body changes;
- in the same area paralysis or paresis of muscles is observed;
- possibly the disappearance of the speech function;
- the inability to recognize one's own disease (if the focus is in the parietal and occipital lobes of the cortex);
- loss of orientation in parts of one's own body;
- loss of visual fields.3 The torsion of the vertebral artery at the neck level causes:hearing loss;
- nystagmus of pupils (twitching in case of deviation to the side);
- double vision in the eyes.
- If the constriction occurred at the site of fusion with the basilar artery, then the clinical symptoms are more severe, since the defeat of the cerebellum predominates:
- impossibility to move;
- impaired gesticulation;
- chanted speech;
- violation of joint movements of the trunk and extremities.
The possibilities of development of compensatory collateral circulation are much higher with the violated patency of extracranial vessels, since there are connecting arteries for blood supply from the other side of the body.
If there is insufficient blood flow in the basilar artery, there are manifestations of visual and stem disorders (violation of breathing and blood pressure).
In defeat of the anterior cerebral artery:
- hemiparesis of the opposite side of the trunk (one-sided loss of sensitivity and movements) more often in the leg;
- slowness of movements;
- increased tonus of flexor muscles;
- loss of speech;
- the inability to stand and walk.
Insult of the brain
Blockage of the middle cerebral artery is characterized by symptoms depending on the defeat of the deep branches (nourish the subcortical nodes) or long (approach the cerebral cortex)
Violation of patency in the middle cerebral artery:
- with a complete blockage of the main trunk there is a deep coma;
- lack of sensitivity and movement in half of the body;
- impossibility to fix a sight on an object;
- loss of visual fields;
- loss of speech;
- lack of ability to distinguish left side from right.
Violation of the passableness of the posterior cerebral artery causes:
- blindness to one or both eyes;
- double vision in the eyes;
- the paresis of the gaze;
- seizures;
- a large tremor;
- disturbed swallowing;
- paralysis from one or both sides;
- violation of breathing and pressure;
- cerebral coma.
If occlusion of the visual-genic artery occurs:
- loss of sensation in the opposite side of the body, face;
- severe pain when touching the skin;
- the inability to localize the stimulus;
- perverted perceptions of light, knocking;
- syndrome of the "thalamic arm" - the shoulder and forearm are bent, the fingers are unbent in the terminal phalanges and are bent at the base.
The broken blood circulation in the zone of the visual thigh, the thalamus cause:
- sweeping movements;
- a large tremor;
- loss of coordination;
- disturbed sensitivity in half of the body;
- sweating;
- early decubitus.
The combination of lesions of several branches causes complex syndromes of loss of sensitivity, false sensations in the limbs. The possibilities of diagnosing ischemic changes depend first of all on the knowledge of the clinical manifestations of vascular disorders by the neurologist.
When are suspected of ONMI?
The above clinical forms and manifestations require careful examination of sometimes not one but a group of physicians of different specialties.
Violation of the cerebral circulation is very likely if the patient exhibits the following changes:
- sudden loss of sensitivity, weakness in the limbs, on the face, especially one-sided;
- acute vision loss, appearance of blindness (one eye or both);
- difficulty in pronunciation, understanding of words and phrases, making suggestions;
- dizziness, loss of balance, impaired coordination of movements;
- confusion of consciousness;
- absence of movements in the limbs;
- intense headache.
Additional examination allows to establish the exact cause of the pathology, the level and localization of the vessel's lesion.
The purpose of diagnosis
Diagnostics are important for choosing a method of treatment. To do this you need:
- to confirm the diagnosis of ONMI and its form;
- to reveal structural changes in the brain tissue, the focus zone, the affected vessel;
- clearly distinguish between ischemic and hemorrhagic forms of stroke;
- on the basis of pathogenesis, establish the type of ischemia for the initiation of specific therapy in the first 3-6 to get into the "therapeutic window";
- to assess the indications and contraindications to drug thrombolysis.
It is practically important to use diagnostic methods in an emergency. But not all hospitals have enough medical equipment for round-the-clock work. The use of echoencephaloscopy and the study of cerebrospinal fluid give up to 20% of errors and can not be used to solve the problem of thrombolysis. The most reliable methods should be used in diagnosis.2Insult of the brain on an MRI
Foci of softening on MRI allow differential diagnosis of hemorrhagic and ischemic strokes
Computer and magnetic resonance tomography allows:
- distinguish the stroke from the volume processes in the brain (tumors, aneurysms);
- accurately determine the size and location of the pathological focus;
- determine the degree of edema, the structure of the ventricles of the brain;
- to reveal extracranial localization of stenosis;
- diagnose vascular diseases that promote stenosis (arteritis, aneurysm, dysplasia, vein thrombosis).
Computer tomography is more accessible, has advantages in the study of bone structures. A magnetic resonance tomography better diagnoses changes in the parenchyma of the brain tissue, the size of the edema.
Echoencephaloscopy can reveal only signs of displacement of median structures in a massive tumor or hemorrhage.
Cerebrospinal fluid rarely gives a small lymphocytosis with ischemia with an increase in protein. More often without changes. If the patient has a hemorrhage, then the appearance of an impurity of blood. And with meningitis - inflammatory elements.
Ultrasound examination of vessels - the method of dopplerography of the arteries of the neck indicates:
- development of early atherosclerosis;
- stenosis of extracranial vessels;
- sufficiency of collateral connections;
- presence and movement of the embolus.
With duplex sonography, you can determine the condition of atherosclerotic plaque and artery walls.Cerebral angiography is carried out with technical capabilities for emergency indications. Usually a more sensitive method is considered in the definition of aneurysms and foci of subarachnoid hemorrhage. Allows you to clarify the diagnosis of pathology, identified by tomography.
Heart ultrasound is used to detect cardioembolic ischemia in cardiac diseases.
A mandatory study of blood coagulability: hematocrit, viscosity, prothrombin time, platelet aggregation and erythrocyte aggregation, fibrinogen.
A survey algorithm
The algorithm of the examination with suspicion of ONMK passes according to the following plan:
examination of a specialist in the first 30-60 minutes after admission of the patient to the hospital, examination of the neurological status, clarification of the anamnesis;
blood sampling and investigation of its coagulability, glucose, electrolytes, enzymes for myocardial infarction, hypoxia level;
in the absence of the possibility of an MRI and CT scan done ultrasound of the brain;
spinal puncture to exclude hemorrhage.
Treatment
The most important in the treatment of cerebral ischemia belongs to the urgency and intensity in the first hours of admission. 6 hours from the beginning of clinical manifestations is called a "therapeutic window". This is the time of the most effective use of the thrombolysis technique for dissolving the blood clot in the vessel and restoring the impaired functions.
Regardless of the type and form of ONMI in the hospital, the following are conducted:
- increased oxygenation (filling with oxygen) of the lungs and normalization of respiratory function (if necessary by translation and ventilation);
- Correction of impaired blood circulation (heart rhythm, pressure);
- normalization of electrolyte composition, acid-base balance;
- reduction of cerebral edema by injection of diuretics, magnesia;
- arresting of excitation, convulsive seizures with special neuroleptic drugs.
To feed the patient appoint a semi-liquid table, if swallowing is impossible, parenteral therapy is calculated. The patient is provided with constant care, prophylaxis of bedsores, massage and passive gymnastics.2LPK after a stroke
Rehabilitation starts from the first days
This allows you to get rid of the negative consequences in the form:
- muscular contractures;
- congestive pneumonia;
- DIC-syndrome;
- thromboembolism of the pulmonary artery;
- lesions of the stomach and intestines.
Thrombolysis is a specific therapy of ONMIK in ischemic type. The method allows to preserve the viability of neurons around the necrosis zone, the return to life of all weakened cells.
Read more about the indications, the procedure for carrying out thrombolysis, you can read in this article.
The introduction of anticoagulants begins with Heparin derivatives (in the first 3-4 days). Contraindicated drugs of this group with:
- high blood pressure;
- peptic ulcer disease;
- diabetic retinopathy;
- bleeding;
The impossibility of organizing regular monitoring of blood coagulability.
After 10 days, they switch to indirect anticoagulants.
To drugs that improve metabolism in neurons, include Glycine, Cortexin, Cerebrolysin, Mexidol. Although they do not appear to be effective in the base of evidence-based medicine, the appointment leads to an improvement in the condition.
Traping of the skull
Decompression trepanation of the skull is performed in the case of increasing edema in the region of the brainstem
Patients may need symptomatic treatment depending on the specific manifestations: anticonvulsant, soothing, anesthetizing.
Antibacterial agents are prescribed to prevent infection of the kidneys and pneumonia.
Prognosis
Data on the prognosis are available only for ischemic infarction, other changes are predecessors indicating an increased risk of stroke.
The most dangerous indicator of death is atherothrombotic and cardioembolic types of ischemia: during the first month of the disease, 15 to 25% of patients die. Lacunar stroke ends deadly only for 2% of patients. The most common causes of death:
in the first 7 days - edema of the brain with compression of vital centers;
up to 40% of all deaths occur in the first month;
after 2 weeks - pulmonary embolism, congestive pneumonia, cardiac pathology.
Invalidity
Only 15% of patients return to work
The presence of signs of disability have:
in a month - up to 70% of patients;
after half a year - 40%;
by the second year - 30%.
Most of all, the rate of recovery is noticeable in the first three months to increase the volume of movements, with the functions of the feet returning faster than the hands. The remaining immobility in the hands after a month is an unfavorable sign. Speech is restored after years.
The process of rehabilitation is most effective at strong-willed efforts of the patient, support of close people. Complicating factors are elderly age, heart disease. Referring to a doctor during the phase of reversible changes will help to avoid serious consequenc
Patient survival time:
1 year - up to 70%;
5 years - 50%;
10 years - 25%.
After this period, they die 16% per year.
2Children.
There is no objective experience of the drug in children.
The drug is contraindicated in children under 12 years of age.
Pharmaceutical characteristics.
tablets are greenish-yellow in color
Composition.
active ingredient: dipyridamole; 1 tablet contains dipyridamole 25 mg;
auxiliary substances: microcrystalline cellulose, calcium stearate, potato starch, talc.
Pharmacotherapeutic group.
Antithrombotic agents. Antiaggregants..
Terms of Storage
Store in a place inaccessible to children in the original packaging, at a temperature not exceeding 25 °C.
Time of validity.
2 years.